While all medications carry some risk, anesthetic medications are among the most dangerous in healthcare if not used correctly. In addition, anesthetists are commonly prescribing, drawing, and administering medications without another provider involved which increases the chance of error. Medication safety is paramount for safe anesthesia practice!
Safe Practices
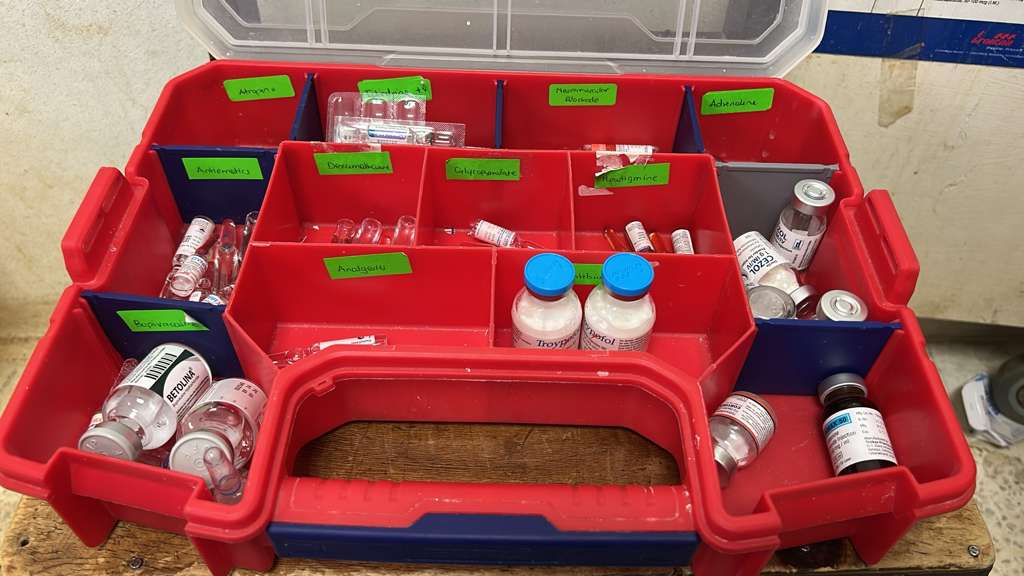
- Organize the anesthesia workstation and your anesthesia drug box. Put similar drugs together to make it easier to access medication by category. Induction drugs may be separated into a bin. Emergency drugs and vasopressors should be grouped in a way that is easy to identify and access. An organized workstation is a safe workstation!
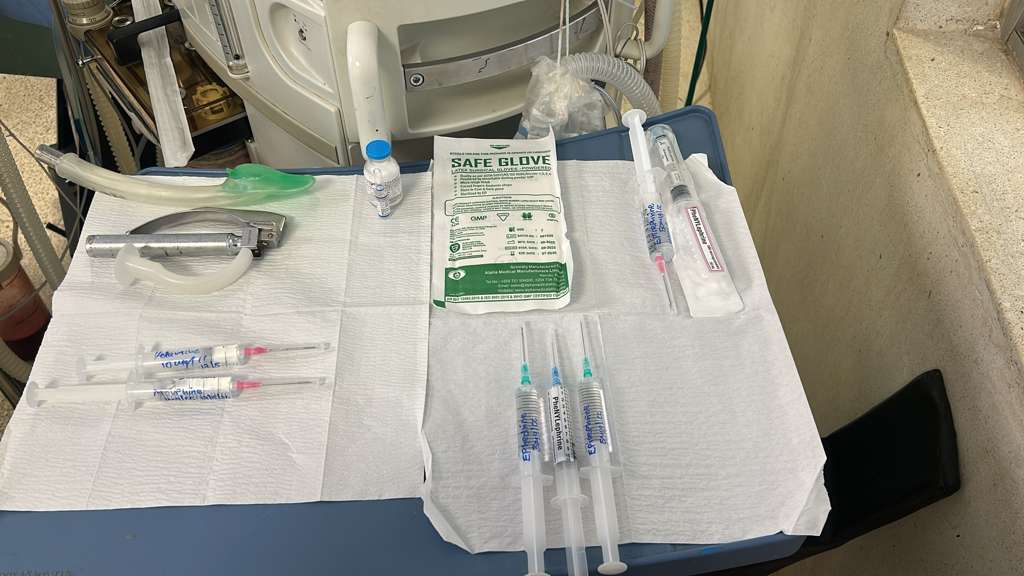
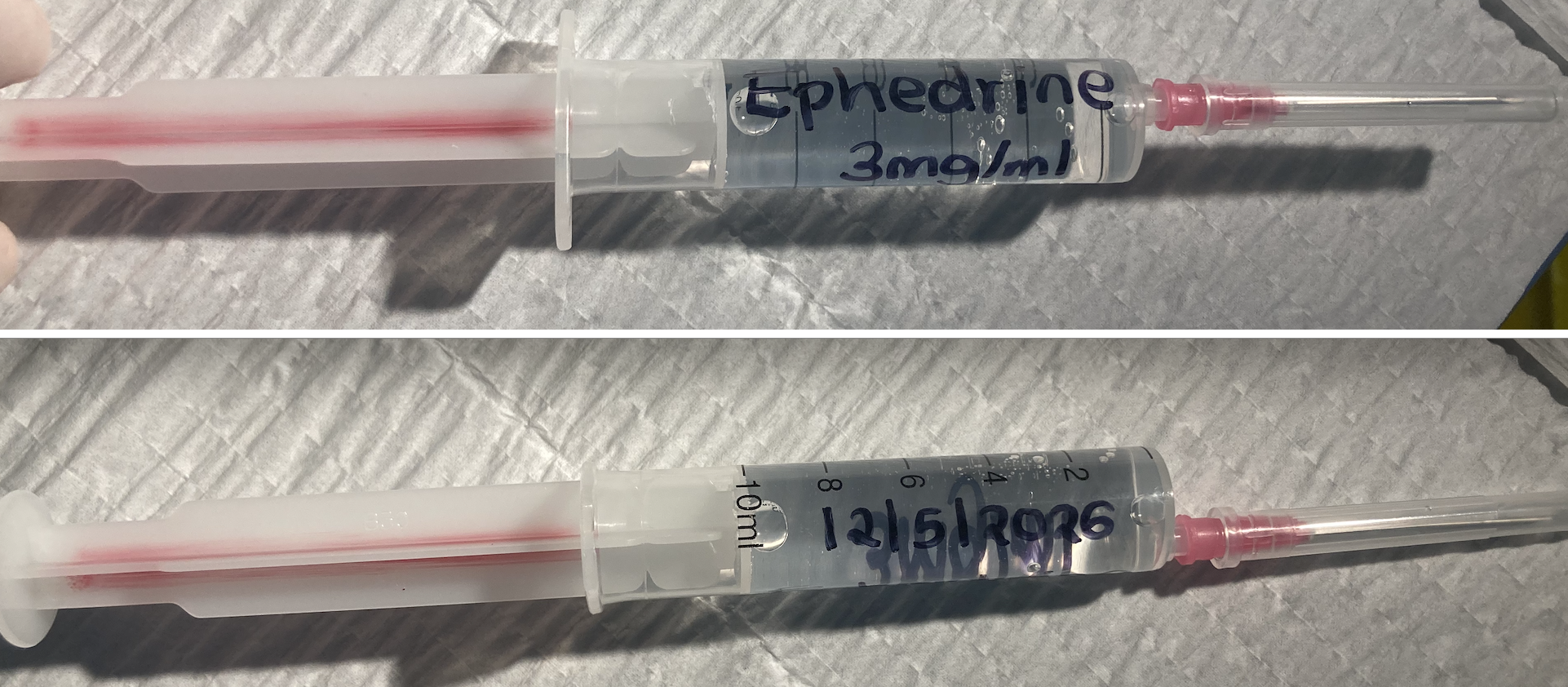
- Label syringes appropriately. Drug name, concentration, and date should be clearly written. Identify high risk medications (i.e., muscle relaxants or adrenaline) with special markings like red ink on the plunger or red tape around the syringe.
- Double-check high-risk medications and infusions. For high-risk medications (see below) and infusions always use a partner to check that the dose, concentration, rate, and administration is correct. For infusions, double-check that the units and concentration of the medication match what is in the syringe. A double-check should be done at every handover, including handover to PACU or ICU/HDU.
- Reduce infectious risk with medications.
- Syringes that come into contact with a patient by pushing into a giving set or IV may not be used on another patient.
- Syringes with medication may not be kept in theatre for more than 24 hours. When in doubt, throw it out. Clear your workstation of medications at the end of the workday.
- Syringes with medications may be kept in refrigeration for up to 7 days but not longer.
- Opened single-use vials and ampules exposed to the environment should not be used for multiple patients
- Medications that require refrigeration (oxytocin, insulin, muscle relaxants) must be replaced quickly and removed from the drug box at the end of the day.
High-Risk Medications
This is a brief, but not exhaustive, list of medications that are used infrequently but are high risk in the theatre environment. If unsure about how to use a medication, be sure to ask a senior or look it up in a trusted resource (UpToDate, OpenEvidence, etc.).
Insulin (regular)
Insulin is used for treating hyperglycemia or hyperkalemia. The concentration from a standard vial is 100IU/mL. The usual dose is 1-10IU, which is 0.01-0.1mL. It should always be administered with a 1mL syringe. Once IV insulin is given, blood glucose should be rechecked within 30-60 minutes.
- May be given as IV bolus, IV infusion, or subcutaneously
- Verify insulin concentration and dose independently with a second practitioner
- Infusion pump misuse (bolus vs. infusion confusion) is a leading cause of insulin fatality
Phenytoin
Occasionally used for seizure management and prophylaxis for neurosurgery in certain brain regions. It can cause bradycardia or cardiac arrest if it is given too quickly. Loading dose is 15-20mg/kg given in 3 doses 2-4 hours apart (maximum 400mg/dose).
- Maximum infusion rate: 50 mg/min in adults (typical dose takes at least 15 minutes); 1 mg/kg/min in children — NEVER bolus
- Continuous ECG and BP monitoring mandatory during infusion
- Stop infusion immediately if PR prolongation, QRS widening >50%, hypotension, or bradycardia occurs
- Administer via large peripheral or central vein — causes severe tissue necrosis if extravasated
Heparin
Used for VTE prophylaxis (prolonged surgery, moderate or high-risk patients) or in vascular surgery to prevent formation of blood clots.
- For VTE prophylaxis, it should be given as 5000 IU subcutaneously and will last 4-6 hours
- For vascular surgery, it may be given as 3000 – 5000 IU IV bolus. This must be done in communication with the surgeon.
Vancomycin
Antibiotic used for certain patients with high-risk or drug-resistant infections. When it is administered too quickly it causes a large histamine release with hypotension and patient discomfort (“red-man syndrome”). Occasionally it is mixed in the surgical field to be used in a wound.
- The IV form should be administered over 1 hour at least, ideally on an infusion pump to prevent rapid administration
